

Short summary: Metformin has been proposed as an “anti-aging drug,” and a major clinical trial is about to get underway to test the idea. In earlier posts in the series, we’ve reviewed the animal data (especially lifespan studies) and human studies on metformin’s effects on a variety of health outcomes, including a flawed observational study suggesting that metformin increases life expectancy in nondiabetic people. This post is focused on trials in which metformin has been studied for its potential in the prevention and treatment of cancer.
Much of the early excitement around potentially using metformin for reasons other than treating diabetes was focused on its potential in cancer prevention in treatment. Several animal studies seemed to show that the drug could either prevent lab animals from getting cancer in the first place, or augment the effects of standard cancer treatments in animals that had developed cancer.
To get initial insights into whether the same might be true in humans, epidemiologists tracked people with diabetes who were taking different drugs to manage their blood glucose, to see if those taking metformin were at lower risk of cancer than diabetics who were taking other drugs instead. Such observational studies initially seemed to confirm that metformin use was linked to lower cancer risk. But as we’ve noted in similar cases (see part two of this series), such findings evaporated when researchers designed studies to take proper account of people who began the study using only metformin but then added on additional drugs as their diabetes got worse during the course of the study, or to correct similar methodological problems.[1],[2],[3]
Fortunately, we aren’t stuck drawing inferences from observational studies. It may come as a surprise, granted all the buzz around TAME, but there have already been hundreds of human clinical trials of metformin for cancer prevention or treatment, either by itself or in combination with standard cancer therapies. This includes over two hundred trials that have already been completed, and another 75 that are either still underway or haven’t gotten off the ground yet.
The fact that you’ve never heard about these trials is not a coincidence: it’s because none of them have led to the kind of result that would garner a headline in the popular press.
To focus our discussion, we should first note that although about two hundred clinical trials have been completed, only about fifty of them have reported their results. We don’t know what happened to the many remaining trials, but it’s safe to assume that if any of them had found metformin to be useful in the prevention or treatment of cancer, the investigators would have taken the trouble to write up the results.
Of the fifty completed studies for which the investigators have reported the results, a number of them don’t actually tell us anything about the benefits or lack thereof of metformin use in cancer. Some of these are studies that were terminated early for uninteresting reasons, such as that the scientists who had set them up couldn’t recruit enough patients to actually run the trial. Others are trials that were completed, but are too preliminary to tell us much either way. For instance, some of them were only checking to make sure that adding metformin to some standard chemotherapy drug didn’t cause a toxic interaction in preparation for a follow-on trial that would actually test for a benefit.
Still other trials merely measured the effect of the drug on levels of insulin or glucose[4],[5],[6] or other markers of glucose metabolism,[7][8] or at effects on immune signaling molecules,[9] without actually looking for an effect on cancer growth or patient survival (or even biomarkers of disease progression). The idea in such trials is usually that either insulin itself or something about abnormal glucose metabolism might be fueling a particular kind of cancer, and the investigators decided that before throwing huge amounts of time and money into a full-sized trial to see if metformin would actually work as a cancer treatment, they would first perform a small study to make sure that metformin could at least lower insulin levels in such cancer patients in the first place.
But that still leaves many trials that have reported results that do tell us something about metformin for the prevention or treatment of cancer — and what they largely tell us is that metformin isn’t useful.
The results of the first really meaningful trial of this kind came out in 2015.[10] Researchers had previously found that metformin inhibited the growth of pancreatic cancers in animal models, by suppressing the tumor cells’ ability to produce energy. Based on those results, 121 people with advanced pancreatic cancer were given the best available chemotherapy, and were then randomly assigned to receive either metformin or a placebo as an add-on treatment.
Patients who took metformin rather than a placebo didn’t survive longer overall, and didn’t even have better chances of surviving for at least six months. If anything, the patients on metformin might have been a little less likely to make it to the six month mark.[10] People on metformin weren’t spared any of the significant side-effects of their chemotherapy, either.
Another trial in pancreatic cancer patients was published the following year,[11] and came to a similar result, despite having used a higher dose of metformin and having confirmed that the drug improved the patients’ glucose metabolism, which the scientists running the trial had expected would correlate with a better cancer outcome. Metformin even failed in the subjects with a genetic variant that correctly predicted a better metabolic response to the drug. And as was seen in the larger trial, there was, if anything, a small hint that people who received metformin might have survived shorter than patients taking placebos.[11] The investigators of this second trial accordingly gave their scientific report the less-than-subtle title “(Ir)relevance of Metformin Treatment in Patients with Metastatic Pancreatic Cancer.”[11]
The most ambitious trial of metformin for cancer was just published this spring (of 2022). In this randomized, placebo-controlled, double-blind Phase III trial, 3,649 women with breast cancer were randomized to receive either metformin or placebo tablets on top of the standard treatment for their subtype of breast cancer.[12] The women in this trial all had cancers that were judged to be high-risk, but had not actually begun to undergo metastasis — the deadly spread that kills most people with cancer. The scientists running this trial also had enough subjects to do special sub-randomizations, depending on what subtype of breast cancer a given woman had and whether she was or wasn’t receiving other chemotherapies. This additional level of random assignment within the trial allowed the scientists to confidently tease out whether there might be some specific context or subgroup of breast cancer patients for whom metformin would be beneficial, even if it wasn’t beneficial for all such patients.
But no matter how they sliced and diced the data, metformin had no impact: women taking metformin didn’t live longer free of cancer after initial treatment, and didn’t do any better on any of the other cancer-related outcomes that the investigators looked at. And some of the more severe toxic effects of treatment were actually more likely to occur in patients taking metformin than in patients who received the placebo.[12]
Several smaller, shorter-term trials of metformin in cancer prevention or treatment have also been completed that were smaller and shorter-term than the trials we reviewed above, but were still able to look for more preliminary signs that metformin might help people with cancer live longer or show some sign of an antitumor effect in people without cancer but who were at risk. A couple of these were studies in breast cancer patients that came back negative, just as the larger trial did.[13],[14] Other studies found that metformin did not make precancerous lesions in the colons of obese men who had suffered previous bouts of colorectal cancer any less dangerous,[15] and that it also didn’t tamp down cancer-related metabolic pathways in biopsies of esophageal tissue from people at high risk of esophageal cancer.[16]
There have also been several completed trials testing the effect of metformin on prostate-specific antigen (PSA) as a possible marker of cancer progression in men with the disease. These trials came to differing results. One trial reported that men with prostate cancer who were given metformin had a slower rise in PSA than is typically seen in men with prostate cancer — but there was no actual control group in the study, so the scientists running the trial couldn’t do a real comparison to confirm that the rise had actually been slowed.[17]
In another uncontrolled trial, PSA rose by less than 20% in seven out of 15 men — but it rose by more than that in the other eight men in the trial, and the authors “acknowledge that post-treatment change in PSA may not be the optimal intermediate end point on the basis of metformin’s proposed mechanism of action.”[18] Meanwhile, an analysis of two other prostate cancer trials found that PSA was higher (that is, potentially, worse) in men who were taking metformin while undergoing treatment than it was in men taking other drugs or in men who weren’t taking any drugs other than their cancer medications — but in this study, the subjects were not randomized to metformin or any of these other side-treatments.[19]
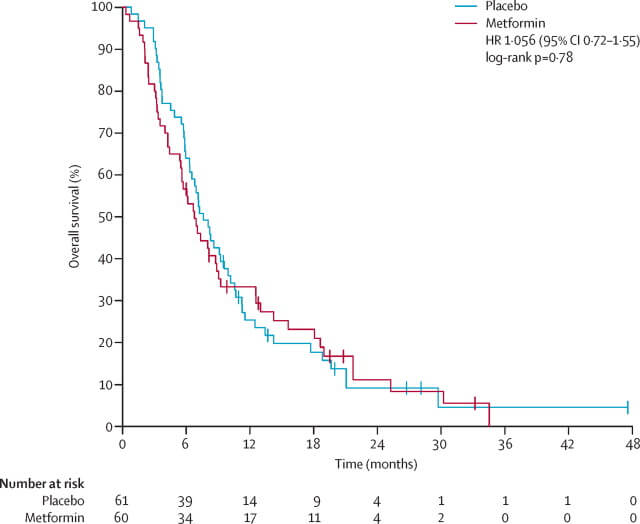
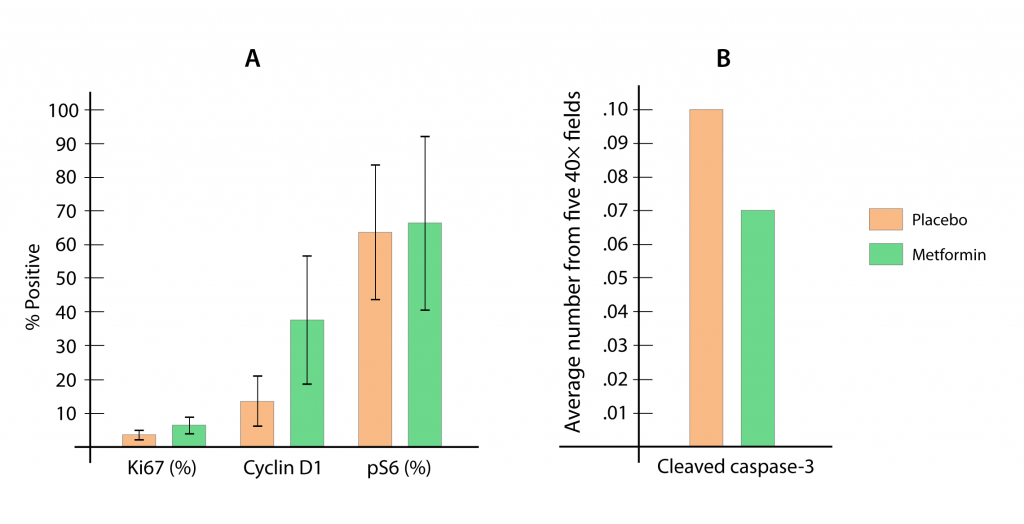
The only true placebo-controlled trial looking at metformin’s effect on PSA in men with prostate cancer found that adding metformin to standard chemotherapy initially modestly lowered the PSA of 40% of the men in the trial, and seemed to improve immune activity. But when they got to the end of the trial, metformin failed to reach the trial’s actual goal, which was to increase the number of men whose PSA was undetectable.[20] The same trial showed that metformin also had no discernable effect on cancer biomarkers in the prostate tissue itself (see the Figure below).[21]
Because the most common kind of endometrial cancer is driven by obesity and insulin resistance, metformin has also been tested as a way to reduce the risk that women with conditions that make them susceptible to this threat will actually develop the disease, or to enhance the effect of other cancer therapies in women who already have it. Six small-to-medium trials were combined into a meta-analysis in an attempt to see if there was a signal anywhere in the noise of these trials.[22]
In the trials for endometrial cancer prevention in women with one set of high-risk conditions, metformin had no effect on the number of cells in the endometrium that were multiplying at a worryingly rapid rate.[22]
A separate high-risk condition for endometrial cancer is treatment with tamoxifen — a drug that is variously used to treat breast cancer; to reduce the risk of breast cancer recurrence after successful breast cancer treatment; and to reduce the risk of developing breast cancer in some high-risk women. Despite tamoxifen’s breast cancer benefits, there is a small risk of endometrial cancer in such women. In a trial of breast cancer survivors who were treated with tamoxifen, adding on metformin did reduce the number of women who went on to develop an abnormally-thick endometrium, which may be an intermediate step along the way to endometrial cancer in tamoxifen-treated women.[22] But even if that’s true, the effect was so small that the chances of this minimal reduction actually translating into fewer of the already-rare cases of endometrial cancers are very slim indeed.
And in women who were being treated for existing endometrial cancer, metformin didn’t increase a woman’s chances of being free of detectable disease at the end of the trials (a “complete response”), or even of having a substantially reduced endometrial tumor mass (a “partial response”).[22]
And finally, one smaller trial suggested that nondiabetic women with a subtype of advanced-stage ovarian cancer who were given metformin seemed to live longer than they were expected to when the trial began.[23] But there were some important limitations to this study. There were only 38 people in the trial, and there was no control group: all the women in the trial were given metformin. These factors make it impossble to determine whether the women in the trial actually had better outcomes than they would have if taking a dummy pill.
All in all, there’s a lot of reason to doubt that metformin will have any effect on all but possibly a couple of cancers — and even in those cancers where it shows some potential, the effect is quite modest if it’s real.
So far we’ve seen the many ways that TAME is likely to disappoint. But no matter what the results of the trial turn out to be, it is still likely to play an important role in the development of longevity therapeutics, moving us toward a future where we can live ever longer with the vigor of our prime. We’ll discuss how TAME will help us in the final post in this series.
Citations:
[1] Farmer RE, Ford D, Mathur R, Chaturvedi N, Kaplan R, Smeeth L, Bhaskaran K. Metformin use and risk of cancer in patients with type 2 diabetes: a cohort study of primary care records using inverse probability weighting of marginal structural models. Int J Epidemiol. 2019 Apr 1;48(2):527-537. doi: 10.1093/ije/dyz005. PMID: 30753459; PMCID: PMC6469299.
[2] Tsilidis KK, Capothanassi D, Allen NE, Rizos EC, Lopez DS, van Veldhoven K, Sacerdote C, Ashby D, Vineis P, Tzoulaki I, Ioannidis JP. Metformin does not affect cancer risk: a cohort study in the U.K. Clinical Practice Research Datalink analyzed like an intention-to-treat trial. Diabetes Care. 2014 Sep;37(9):2522-32. doi: 10.2337/dc14-0584. Epub 2014 Jun 4. PMID: 24898303.
[3] Stevens RJ, Ali R, Bankhead CR, Bethel MA, Cairns BJ, Camisasca RP, Crowe FL, Farmer AJ, Harrison S, Hirst JA, Home P, Kahn SE, McLellan JH, Perera R, Plüddemann A, Ramachandran A, Roberts NW, Rose PW, Schweizer A, Viberti G, Holman RR. Cancer outcomes and all-cause mortality in adults allocated to metformin: systematic review and collaborative meta-analysis of randomised clinical trials. Diabetologia. 2012 Oct;55(10):2593-2603. doi: 10.1007/s00125-012-2653-7. Epub 2012 Aug 10. Erratum in: Diabetologia. 2012 Dec;55(12):3399-400. PMID: 22875195.
[4] Brown JC, Zhang S, Ligibel JA, Irwin ML, Jones LW, Campbell N, Pollak MN, Sorrentino A, Cartmel B, Harrigan M, Tolaney SM, Winer EP, Ng K, Abrams TA, Sanft T, Douglas PS, Hu FB, Fuchs CS, Meyerhardt JA. Effect of Exercise or Metformin on Biomarkers of Inflammation in Breast and Colorectal Cancer: A Randomized Trial. Cancer Prev Res (Phila). 2020 Dec;13(12):1055-1062. doi: 10.1158/1940-6207.CAPR-20-0188. Epub 2020 Aug 28. PMID: 32859615; PMCID: PMC7718298.
[5] Brown JC, Zhang S, Ligibel JA, Irwin ML, Jones LW, Campbell N, Pollak MN, Sorrentino A, Cartmel B, Harrigan M, Tolaney SM, Winer EP, Ng K, Abrams TA, Sanft T, Douglas PS, Hu FB, Fuchs CS, Meyerhardt JA. Effect of Exercise or Metformin on Biomarkers of Inflammation in Breast and Colorectal Cancer: A Randomized Trial. Cancer Prev Res (Phila). 2020 Dec;13(12):1055-1062. doi: 10.1158/1940-6207.CAPR-20-0188. Epub 2020 Aug 28. PMID: 32859615; PMCID: PMC7718298.
[6] Patterson RE, Marinac CR, Sears DD, Kerr J, Hartman SJ, Cadmus-Bertram L, Villaseñor A, Flatt SW, Godbole S, Li H, Laughlin GA, Oratowski-Coleman J, Parker BA, Natarajan L. The Effects of Metformin and Weight Loss on Biomarkers Associated With Breast Cancer Outcomes. J Natl Cancer Inst. 2018 Nov 1;110(11):1239-1247. doi: 10.1093/jnci/djy040. PMID: 29788487; PMCID: PMC6235688.
[7] Samson SL, Gu F, Feldt-Rasmussen U, Zhang S, Yu Y, Witek P, Kalra P, Pedroncelli AM, Pultar P, Jabbour N, Paul M, Bolanowski M. Managing pasireotide-associated hyperglycemia: a randomized, open-label, Phase IV study. Pituitary. 2021 Dec;24(6):887-903. doi: 10.1007/s11102-021-01161-4. Epub 2021 Jul 18. PMID: 34275099; PMCID: PMC8550309.
[8] Yeh HC, Maruthur NM, Wang NY, Jerome GJ, Dalcin AT, Tseng E, White K, Miller ER, Juraschek SP, Mueller NT, Charleston J, Durkin N, Hassoon A, Lansey DG, Kanarek NF, Carducci MA, Appel LJ. Effects of Behavioral Weight Loss and Metformin on IGFs in Cancer Survivors: A Randomized Trial. J Clin Endocrinol Metab. 2021 Sep 27;106(10):e4179-e4191. doi: 10.1210/clinem/dgab266. PMID: 33884414; PMCID: PMC8475239.
[9] Karivedu V, Yaniv Y, Asman M, Palackdharry SM, Gulati S, Jandarov R, Sadraei NH, Takiar V, Wise-Draper TM. Metformin treatment of locally advanced head and neck squamous cell carcinoma (LAHNSCC) patients induces an anti-tumorigenic immune response. J Clin Oncol. 2019 May 20; 37 (15 Suppl):6037-6037 DOI: 10.1200/JCO.2019.37.15_suppl.6037.
[10] Kordes S, Pollak MN, Zwinderman AH, Mathôt RA, Weterman MJ, Beeker A, Punt CJ, Richel DJ, Wilmink JW. Metformin in patients with advanced pancreatic cancer: a double-blind, randomised, placebo-controlled phase 2 trial. Lancet Oncol. 2015 Jul;16(7):839-47. doi: 10.1016/S1470-2045(15)00027-3. Epub 2015 Jun 8. PMID: 26067687.
[11] Reni M, Dugnani E, Cereda S, Belli C, Balzano G, Nicoletti R, Liberati D, Pasquale V, Scavini M, Maggiora P, Sordi V, Lampasona V, Ceraulo D, Di Terlizzi G, Doglioni C, Falconi M, Piemonti L. (Ir)relevance of Metformin Treatment in Patients with Metastatic Pancreatic Cancer: An Open-Label, Randomized Phase II Trial. Clin Cancer Res. 2016 Mar 1;22(5):1076-85. doi: 10.1158/1078-0432.CCR-15-1722. Epub 2015 Oct 12. PMID: 26459175.
[12] Goodwin PJ, Chen BE, Gelmon KA, Whelan TJ, Ennis M, Lemieux J, Ligibel JA, Hershman DL, Mayer IA, Hobday TJ, Bliss JM, Rastogi P, Rabaglio-Poretti M, Mukherjee SD, Mackey JR, Abramson VG, Oja C, Wesolowski R, Thompson AM, Rea DW, Stos PM, Shepherd LE, Stambolic V, Parulekar WR. Effect of Metformin vs Placebo on Invasive Disease-Free Survival in Patients With Breast Cancer: The MA.32 Randomized Clinical Trial. JAMA. 2022 May 24;327(20):1963-1973. doi: 10.1001/jama.2022.6147. PMID: 35608580; PMCID: PMC9131745.
[13] Pimentel I, Lohmann AE, Ennis M, Dowling RJO, Cescon D, Elser C, Potvin KR, Haq R, Hamm C, Chang MC, Stambolic V, Goodwin PJ. A phase II randomized clinical trial of the effect of metformin versus placebo on progression-free survival in women with metastatic breast cancer receiving standard chemotherapy. Breast. 2019 Dec;48:17-23. doi: 10.1016/j.breast.2019.08.003. Epub 2019 Aug 22. PMID: 31472446.
[14] Nanni O, Amadori D, De Censi A, Rocca A, Freschi A, Bologna A, Gianni L, Rosetti F, Amaducci L, Cavanna L, Foca F, Sarti S, Serra P, Valmorri L, Bruzzi P, Corradengo D, Gennari A; MYME investigators. Metformin plus chemotherapy versus chemotherapy alone in the first-line treatment of HER2-negative metastatic breast cancer. The MYME randomized, phase 2 clinical trial. Breast Cancer Res Treat. 2019 Apr;174(2):433-442. doi: 10.1007/s10549-018-05070-2. Epub 2018 Dec 7. PMID: 30536182.
[15] Zell JA, McLaren CE, Morgan TR, Lawson MJ, Rezk S, Albers CG, Chen WP, Carmichael JC, Chung J, Richmond E, Rodriguez LM, Szabo E, Ford LG, Pollak MN, Meyskens FL. A Phase IIa Trial of Metformin for Colorectal Cancer Risk Reduction among Individuals with History of Colorectal Adenomas and Elevated Body Mass Index. Cancer Prev Res (Phila). 2020 Feb;13(2):203-212. doi: 10.1158/1940-6207.CAPR-18-0262. Epub 2019 Dec 9. PMID: 31818851; PMCID: PMC8025666.
[16] Chak A, Buttar NS, Foster NR, Seisler DK, Marcon NE, Schoen R, Cruz-Correa MR, Falk GW, Sharma P, Hur C, Katzka DA, Rodriguez LM, Richmond E, Sharma AN, Smyrk TC, Mandrekar SJ, Limburg PJ; Cancer Prevention Network. Metformin does not reduce markers of cell proliferation in esophageal tissues of patients with Barrett’s esophagus. Clin Gastroenterol Hepatol. 2015 Apr;13(4):665-72.e1-4. doi: 10.1016/j.cgh.2014.08.040. Epub 2014 Sep 15. PMID: 25218668; PMCID: PMC4362887.
[17] Rothermundt C, Hayoz S, Templeton AJ, Winterhalder R, Strebel RT, Bärtschi D, Pollak M, Lui L, Endt K, Schiess R, Rüschoff JH, Cathomas R, Gillessen S. Metformin in chemotherapy-naive castration-resistant prostate cancer: a multicenter phase 2 trial (SAKK 08/09). Eur Urol. 2014 Sep;66(3):468-74. doi: 10.1016/j.eururo.2013.12.057. Epub 2014 Jan 4. PMID: 24412228.
[18] Galsky MD, Shahin M, Jia R, Shaffer DR, Gimpel-Tetra K, Tsao CK, Baker C, Leiter A, Holland J, Sablinski T, Mehrazin R, Sfakianos JP, Acon P, Oh WK. Telemedicine-Enabled Clinical Trial of Metformin in Patients With Prostate Cancer. JCO Clin Cancer Inform. 2017 Nov;1:1-10. doi: 10.1200/CCI.17.00044. PMID: 30657386.
[19] Roy S, Malone S, Grimes S, Morgan SC. Impact of Concomitant Medications on Biochemical Outcome in Localised Prostate Cancer Treated with Radiotherapy and Androgen Deprivation Therapy. Clin Oncol (R Coll Radiol). 2021 Mar;33(3):181-190. doi: 10.1016/j.clon.2020.09.005. Epub 2020 Sep 29. PMID: 32994091.
[20] Bilusic M, Toney NJ, Donahue RN, Wroblewski S, Zibelman M, Ghatalia P, Ross EA, Karzai F, Madan RA, Dahut WL, Gulley JL, Schlom J, Plimack ER, Geynisman DM. A randomized phase 2 study of bicalutamide with or without metformin for biochemical recurrence in overweight or obese prostate cancer patients (BIMET-1). Prostate Cancer Prostatic Dis. 2022 Jan 25. doi: 10.1038/s41391-022-00492-y. Epub ahead of print. PMID: 35079115.]
[21] Nguyen MM, Martinez JA, Hsu CH, Sokoloff M, Krouse RS, Gibson BA, Nagle RB, Parnes HL, Cordova C, Chow HS. Bioactivity and prostate tissue distribution of metformin in a preprostatectomy prostate cancer cohort. Eur J Cancer Prev. 2018 Nov;27(6):557-562. doi: 10.1097/CEJ.0000000000000394. PMID: 28692586; PMCID: PMC5756696.
[22] Prodromidou A, Lekka S, Fotiou A, Psomiadou V, Iavazzo C. The evolving role of targeted metformin administration for the prevention and treatment of endometrial cancer: A systematic review and meta-analysis of randomized controlled trials. J Gynecol Obstet Hum Reprod. 2021 Nov;50(9):102164. doi: 10.1016/j.jogoh.2021.102164. Epub 2021 May 13. PMID: 33992830.
[23] Brown JR, Chan DK, Shank JJ, Griffith KA, Fan H, Szulawski R, Yang K, Reynolds RK, Johnston C, McLean K, Uppal S, Liu JR, Cabrera L, Taylor SE, Orr BC, Modugno F, Mehta P, Bregenzer M, Mehta G, Shen H, Coffman LG, Buckanovich RJ. Phase II clinical trial of metformin as a cancer stem cell-targeting agent in ovarian cancer. JCI Insight. 2020 Jun 4;5(11):e133247. doi: 10.1172/jci.insight.133247. PMID: 32369446; PMCID: PMC7308054.
See also the other posts in this series:
- Part 1: on the animal data on metformin and aging;
- Part 2: on some human studies on metformin, including a flawed observational study that created the illusion that diabetics on metformin actually live longer than people without diabetes;
- Part 4: on human studies on metformin and age-related cognitive decline and dementia; and
- Part 5: on the backstory on TAME and how it might impact the push for longevity therapeutics.
- Addendum: More Studies on Metformin and Survival
- Addendum: Monkeying With the Clocks Via Metformin